
BANGALORE ADVANCED UROLOGY
Reconstructive Urology
Safe. Affordable. Ethical Treatments
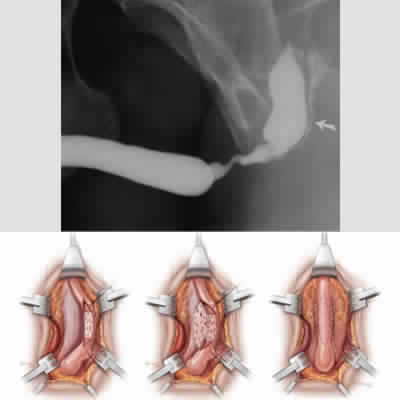
Urethroplasty
A urethral stricture occurs when scarring narrows the tube that carries urine out of your body. Urethral stricture restricts the flow of urine from the bladder and can cause a variety of medical problems in the urinary tract, including inflammation or infection.
Urethroplasty involves surgically removing the narrowed section of your urethra or enlarging it. The procedure to cure urethral stricture may also involve reconstruction of the surrounding tissues. Tissues from other areas of the body, such as your skin or mouth (buccal mucosa ), may be used as a graft during reconstruction.
There are various types of urethroplasty procedures for urethral stricture.
- Bulbar Anastomotic
- Anastomitoc Urethroplasty – Membranous urethra
- Augmented Urethroplasty (Barbagli)
- Ventral Onlay
- Augmented Anastomosis
- Substitution Urethroplasty
If done beautifully, a well-done urethroplasty of urethral stricture can save you years in medical costs and procedures.
The first surgery is the best surgery. So, be aware of choosing a surgeon or surgery which promises you the easy way out, may not be a prudent decision.
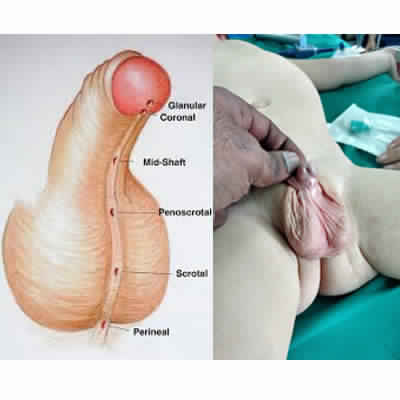
Hypospadias repair
Hypospadias, unlike urethral stricture, is a condition in which the opening of the urethra is on the underside of the penis, instead of at the tip. The urethra is the tube through which urine drains from your bladder and exits your body
You may feel distressed if your son is born with hypospadias. However, hypospadias is common and doesn’t cause difficulty in caring for your infant. In fact, surgery usually restores the normal appearance of your child’s penis. With successful treatment of hypospadias, most males can eventually have normal adult sexual function.
During surgery, we use tissue grafts from the foreskin or from the inside of the mouth to reconstruct the urinary channel in the proper position, correcting the hypospadias . Rarely, the repair may require two or more surgeries
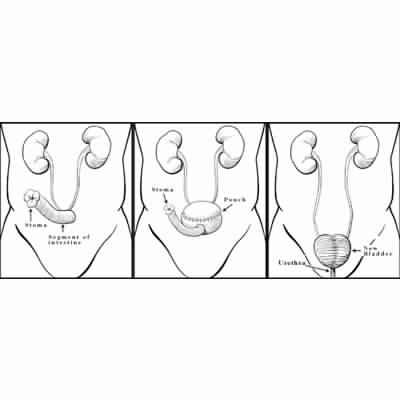
Urinary Diversions
When the urinary bladder is removed (due to cancer, other medical condition, urethral stricture or because the organ no longer works), another method must be devised for urine to exit the body. Urinary reconstruction and diversion is a surgical method to create a new way for you to pass urine.
There are three main types of urinary diversion surgeries
- Ileal Conduit Urinary Diversion
- Continent cutaneous reservoir
- Neobladder to Urethra Diversion
Ileal Conduit Urinary Diversion
With this procedure, the ureters drain freely into part of the ileum (the last segment of the small intestine). The end of the ileum into which the ureters drain is then brought out through an opening in the abdominal wall. This opening, called a stoma, is covered with a bag that gathers the urine as it drains from the ileal conduit.
Advantages:
The advantages of the Ileal Conduit Urinary Diversion surgery are:
- It is a relatively simple surgery.
- It requires less surgical time (compared with other surgical methods).
- There is no need for occasional catheterization (use of a tube to drain the urine)
Disadvantages:
The disadvantages of the Ileal Conduit Urinary Diversion are:
- There is a change in body image.
- It uses an external bag to collect urine, which might leak or have odors.
- Urine could back up into the kidneys, causing infections, stone formation in some patients, and organ damage over time.
Pouch Reservoir
This procedure most closely mimics the storage function of a urinary bladder. With this procedure, a small part of the small intestine is made into a reservoir or pouch, which is connected to the urethra. The ureters are repositioned to drain into this pouch. As with the Indiana Pouch, this downward flow of urine from the kidneys into the pouch helps prevent urine back up, which helps protect the kidneys from infection. Urine is able to pass from the kidney, to the ureters, to the pouch, and through the urethra in a manner similar to the normal passing of urine. To be a candidate for this surgical procedure, there must be a low risk of cancer recurrence in the urethra, and patients must be able to pass a catheter into the urethra to empty the pouch if necessary.
Advantages:
The advantages of the Neobladder to Urethra Diversion are:
- The process of urination most closely matches normal urination.
No stoma is needed. - The kidneys are protected from urine back up and infection.
Disadvantages:
The disadvantages of the Neobladder to Urethra Diversion are:
- Surgery time is slightly longer than the Ileal Conduit Urinary Diversion procedure.
- Urinary incontinence (leakage of urine) is normal after surgery — while regaining control of urination — but might last up to six months. Also, about 20 percent of patients during the night and 5 percent to 10 percent of patients during the day are incontinent, requiring the wearing of a pad.
- Despite the surgery, some patients might not be able to empty their bladder well and will need to perform occasional catheterization (passing tubing through the urethra into the pouch every four to six hours) for a prolonged period of time after surgery and perhaps permanently.
Neobladder to Urethra Diversion
With this type of surgery, a reservoir or pouch is made out of a portion of the large intestine (the ascending colon on the right side of the abdomen) and a portion of the ileum (the last segment of the small intestine). The ureters are repositioned to drain into this pouch. The urine flows freely in a downward direction from the kidneys into the pouch. This positioning prevents urine from backing up into the kidneys, which protects the kidneys from infection. A short piece of small intestine is then brought out through a small opening in the abdominal wall (a stoma). Unlike the Ileal Conduit, no external bag is needed, and the stoma is very small and can be covered with an adhesive bandage. Instead, a one-way valve is surgically created to keep the urine inside the pouch. Several times a day, usually every four to six hours, a small, thin catheter must be passed through the stoma and into the pouch to empty the urine. An adhesive bandage is worn over the stoma at all other times (when not actively emptying the pouch). Catheters are washed with soap and water after each use. The catheters do not have to be sterilized. They can be taken on trips or social events and simply stored in a zip lock bag.
Advantages:
The advantages of the Indiana Pouch Reservoir surgery are:
- Urine is kept inside the body, in the reservoir, until it is ready to be emptied.
- There is no odor.
- The risk of urine leaking is minimal.
- The small stoma can be covered with an adhesive bandage.
- The risk of reflux (back up) of urine into the kidneys is lessened, lowering the risk of infection.
Disadvantages:
The disadvantages of the Indiana Pouch are:
- The surgical time is longer compared with the Ileal Conduit.
- There is the need for occasional catheterization (the passing of tubing into the stoma to empty the pouch), every four to six hours.
Ileal Ureter
A ureteral stricture dissimilar to urethral stricture is characterized by a narrowing of the ureteral lumen, causing functional obstruction
Partial or complete ureteral replacement with small bowel is indicated as a second-line treatment after failure of ureter-sparing surgery.
Unlike urethral stricture, Ureteral narrowing varies in location and length, and thus in their various treatment options. Once the decision is made to perform reconstruction of the ureter, we offer the best approach to reconstruction of the ureter. For long ureteral strictures, we perform the ileal ureter replacement unlike urethral srticture.
Ureteroureterostomy is conceptually the simplest form of ureteral reconstruction of the upper, middle, or lower short segment defect, the distal ureteric defect can be managed successfully by ureterovesical reimplantation combined with anti-reflux technique, the longer ones are usually managed by Boari’s flap and in rare situations, by downward mobilization of the involved kidney, renal autotransplantation or urinary diversion .Moreover, extensive ureteral defects may need partial or total ureteral replacement by ileal loop or pedicled bowel segments.
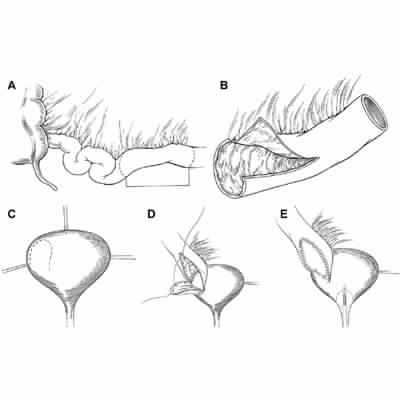
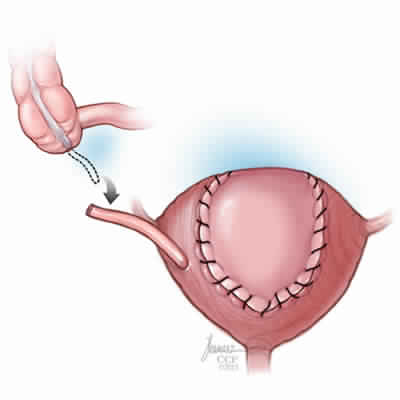
Augmentation cystoplasty
Augmentation cystoplasty, also known as bladder augmentation, is a surgery to make the bladder larger. (The bladder is the organ that holds urine.)
Many patients, augmentation cystoplasty can provide a safe functional reservoir that allows for urinary continence and prevention of upper tract deterioration. Both neuropathic and non-neuropathic causes for severe bladder dysfunction exist in pediatric and adult populations.
Decreased bladder capacity or abnormal compliance may manifest as debilitating urgency, frequency, incontinence, recurrent urinary tract infections (UTIs), pyelonephritis, or progressive renal insufficiency.
After making the incision in the abdomen, the surgeon cuts open the bladder at the top to prepare it for enlarging.
The surgeon then removes a section of the small or large intestine ; detubularizes (cuts open) that link of bowel , and attaches it to the top of the bladder. The bladder and bowel are then sewn together to make the bladder larger.
Send us Your Concerns
When you write to us
Kindly provide the following information
- Your name
- Contact number
- Your location
- The specific message to assist you better.
- Are you on hormonal therapy ?
- Have you undergone any surgery for the same problem ?